



By Natasha Mohr
Hyperkeratosis, corns, athletes foot, nail fungus and cracked heels… while you are not a podiatrist, chances are good that you spend at least part of your day dealing with the wide array of maladies related to feet. To help you better help your patients take care of those hardworking extremities, we have some creative tips and tricks you can share for getting les pieds back on the road. From beating back bacteria to using fillers and neurotoxins to ease metatarsalgia – we’ve got you covered!
Banish Bacteria
You’re already telling your patients that having clean, dry feet has to be part of their regular hygiene routine. You’re already telling them that they need to remove wet or sweaty socks and shoes right away and to towel dry between their toes thoroughly after washing their feet. But they should also be using a body wash designed to kill 99.9% of P. acnes and S. Aureus without risking barrier disruption.
For his patients in Omaha, NE, Dr. Joel Schlessinger makes a point of helping his patients understand that proper cleaning is the very first step to achieving healthy skin. “Sodium hypochlorite delivered via bleach baths is known to be antimicrobial, anti-inflammatory and anti-aging. Bleach baths are clinically effective for Atopic Dermatitis and Staph aureus decolonization. CLn Skin Care has introduced washes formulated with sodium hypochlorite plus surfactants and their propriety technology allows for safe, easy delivery of the benefits with no barrier disruption,” Schlessinger says.
“Using this wash is very simple. Patients wet the affected area(s), then they work the product into a lather and massage into the skin, hair or nails for 1 to 3 minutes (depending on the area of the body) and rinse thoroughly. Patients should then apply moisturizer or other products as needed. Most CLn products can be used daily, but dryness does occur, patients should reduce usage to every other day. The CLn products are a highly effective, very affordable alternative to prescriptions for many patients. I recommend it for eczema/atopic dermatitis, folliculitis and skin infections, acne, athlete’s foot, dandruff and even ringworm. Because it is inexpensive and incredibly easy to use, patients are highly compliant and see wonderful results” says Schlessinger.
There have been two papers published on CLn products. The first two sets of images below were included in Caitriona Ryan, Richard E. Shaw, Clay J. Cockerell, Shari Hand Fred E. Ghali “Novel Sodium Hypochlorite Cleanser Shows Clinical Response and Excellent Acceptability in the Treatment of Atopic Dermatitis.” Ped Derm, 70, no. 3, May/June 2013, Pages 308 – 315. The third set of image is from Bohaty, Benjamin, Adelaide Hebert, Amy Paller, Dennis West, Gil Abramovici, and Kathryn Durham. “A novel new sodium hypochlorite formulated wash as an adjunctive approach to the management of pediatric subjects with moderate to severe atopic dermatitis colonized with Staphylococcus aureus.” J Am Acad Dermatol 70, no. 5 Suppl 1 (2014).

10 y/o, on Cyclosporine, baseline vs. 10 weeks after CLn with no antibiotics used
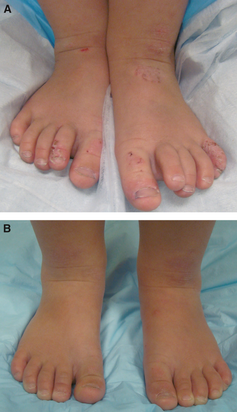
2 y/o with eczema & recurrent staph cellulitis – Baseline vs. 8 weeks on CLn


12 y/o baseline -staph culture positive, (0 weeks) vs. visit 2 (2 weeks) on CLn, no antibiotics used
Treating Palmoplantar Skin
Taking an unorthodox approach to treating palmoplantar skin is Dr. Matt Zirwas, of Columbus, OH. He asks patients to use hair removal cream on the soles of their feet. “Hyperkeratosis is keratin,” he says. “Hair removal cream is the ONLY thing that quickly dissolves keratin. It has been demonstrated that it increases penetration of steroid by over 10 times on palmoplantar skin. So, when I see a palmar or plantar dermatitis, I have them get hair removal cream and do the following regimen daily: Apply hair removal cream to damp skin on palm or sole, leave it on for 3 minutes, firmly wipe off, then immediately apply clobetasol cream.” Zirwas warns his colleagues to give patients a heads up that “it will burn for the 3 minutes they have it on.” The maintenance plan is simple. “Once they are better, they need to continue to follow the regimen 2 days per week to remain clear.”
Calluses and Cracks Be Gone
Most patients are not dealing with anything so painful or difficult to treat as palmoplantar skin, but do have their fair share of tough calluses and cracked heals.
If you aren’t into suggesting particular products they can purchase, you can always recommend one of the seemingly hundreds of DIY remedies to be found online. Thankfully, the tiny toothless carp fish pedicure has fallen by the wayside, but there are still some beneficial remedies to be found ranging from soaking one’s feet in a bath of sea salt water in preparation for the pumice stone to rubbing on olive oil and wearing socks to bed.
Also, patients need to be aware that they have to be careful when they buy shoes. Shoe shopping in the afternoon because your feet swell, wearing breathable fabrics and having your foot measured by a professional are all essential keys to preventing calluses, cracks and most other foot-pain issues. Reminding patients of this should certainly be a starting point in the conversation.
If you are not product recommendation averse, there are some highly effective items that you may wish to consider recommending to patients for addressing minor to moderate calluses and heel cracks. Dr. Joel Schlessinger often recommends NeoStrata Company and Glytone. Both brands are well-known for being based in quality science and for producing highly effective products.
NeoStrata’s Problem Dry Skin Cream (PDS) is formulated with 20% Alpha Hydroxy Acids (AHAs) with high tolerability, maltobionic acid, vitamin E and an amphoteric formulation to reduce redness. In addition to being highly effective for treating calluses on feet, it is also a wonderful product to help soften psoriasis plaques.
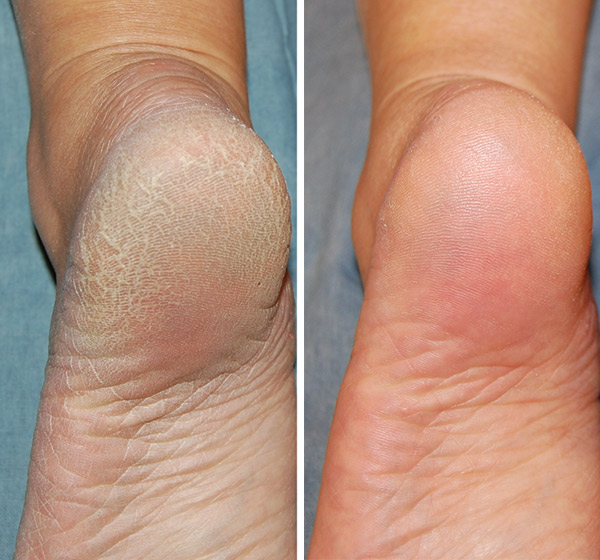
NeoStrata Problem Dry Skin Cream – Before & After Images – 3 weeks
Glytone’s Ultra Softening Heel and Elbow Cream is made with highly concentrated Glycolic Acid (29.5 PFAV™*), Glycerin and protective emollients to retexturize, exfoliate, moisturize, smooth, and polish the skin. The high level of Glycolic Acid helps to dissolve the dead keratinocytes leaving behind a renewed skin surface.
At $42 and $54 respectively, these are excellent product options for patients who need a moderate treatment product that goes beyond simple hydration.
Bring on the Stilettos!
Lastly, we wish to address one of the foot pain issues with which podiatrists have been historically most likely to deal: high-heel induced foot pain. Hammer toes, bunions and pump-bump are all issues caused by long-term wearing of high heels and are best left to the expertise of a podiatrist. But the most common foot pain comes on the front end of wearing heels, long before any lasting foot deformities take root. We’re taking about the inflammation that occurs from the added pressure placed on the balls of your feet from the unnatural foot position created by wearing heels. Known as ‘metatarsalgia’ and experienced by every person who has worn heels in the history of wearing heels – a solution can be found right in the dermatology office.
Dr. Suneel Chilukuri, in Houston, TX, has created a protocol with which he is seeing wonderful, long-term results. “We call it the ‘Cinderella Treatment’, ” he says. “It is a new protocol for treating pain on the ball of the foot, which often occurs when wearing high heels. I use a combination of a radiofrequency / ultrasound device (BTL Exilis Ultra), hyaluronic acid filler and neuromodulator to relieve this pain. With this protocol, I am seeing long-term results with pain-free, happy patients.”
This sounds incredibly promising, Dr. Chilukuri! We look forward to hearing more about this – and perhaps seeing a live patient demonstration – at this year’s Cosmetic Surgery Forum. Be sure to join us!
Leave a Comment